
Ivan Sergeevich Moiseevgraduated from the First St. Petersburg State Medical University.
Since 2013, scientific interests have been focused onreducing mortality from complications of hematopoietic cell transplantation and graft-versus-host disease. Since 2015, he has become the head of the Department of Hematology and Transplantation for Adults at the Research Institute of DogiT named after. R. M. Gorbacheva. Since 2017, he has been working as the Deputy Director for Science of the Research Institute of DoGiT named after V.I. R. M. Gorbacheva. In 2019, he defended his doctoral dissertation on the topic of prevention and treatment of graft-versus-host disease. Since 2021 - Professor of the Department of Oncology, Hematology and Transplantology at the University. I.P. Pavlova.
Author and co-author of more than 100 publications coveringvarious aspects of clinical hematology and hematopoietic stem cell transplantation. He is an active member of the European Association for Bone Marrow Transplantation (EBMT) and Secretary of the Working Group on Transplant Complications.
"CAR-T is used in situations where there is no alternative"
- At the Research Institute. Gorbacheva begin the introduction of a new type of therapy against cancer - CAR-T. Tell us what its essence is and for what diagnoses it is used?
—We have passed all the validation stages, and this year the clinical testing of the method begins - we will treat patients as part of a joint project with the N.N. N.N. Petrov.
The technology is based on geneticallymodified cells of the patient himself. Genetic modification involves combining one protein from human B cells and a second protein from human T cells, plus an additional boosting protein. Such a triple structure does not exist in nature.
This technology was first developed in Israelback in the early 1990s, but only found clinical use in the last five years, because the key factor was the presence of this signal-enhancing protein, which allowed the T cells to work to their full potential. All other modifications before that were clinically not very effective.
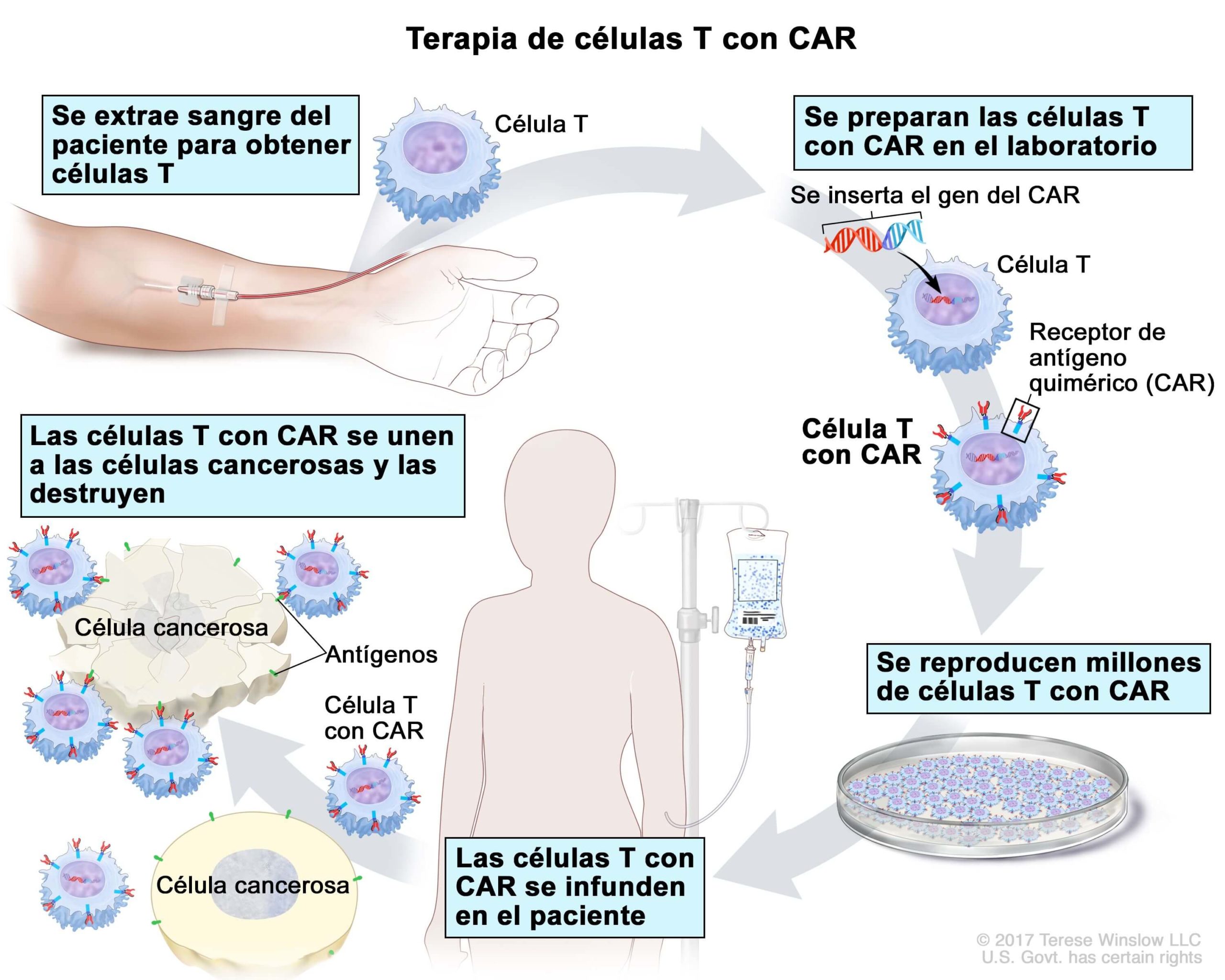 Scheme of work of CAR-T therapy. Source: cancer.gov
Scheme of work of CAR-T therapy. Source: cancer.gov
The problem with this therapy is thatT cells directed against a target kill the target cell in any case, even if it is normal and only potentially dangerous. Therefore, the limitation of this therapy today is the so-called off-target effect, when neurotoxicity occurs in relation to the patient's normal tissues. And here it is precisely B-cell tumors that stand out - leukemia and lymphomas, because even if the drug destroys all the patient’s B-cells, the patient will be able to survive this (blood transfusions and immunoglobulins will help) and recover with healthy cells.
If we talk about solid tumors - for example,cancer of the gastrointestinal tract, human epithelial cells are found everywhere. And if a targeted drug attacks all the epithelial cells of the body, it will result in toxic shock. Therefore, today there is a rather narrow range of targets for which this is possible for the current technology.
solid tumors- solid, clearly limited growth fromown mature (differentiated) tissue or immature (rudimentary, undifferentiated) tissue. They can appear in any of the internal organs or organ systems. There are benign and malignant.
Hemoblastoses- tumor (neoplastic) diseases of hematopoietic and lymphatic tissue. They are divided into systemic diseases - leukemia, as well as regional ones - lymphomas.
For which patients will this treatment be applied?
— Our first stage of the project is related to adult patients. For children today, therapy is used at the Dima Rogachev Institute in Moscow (NMIC DGOI named after Dmitry Rogachev - "High Tech").
- How is the therapy introduced into the body - is it an injection, a pill or something?
“This is a small sachet for intravenous infusion, which usually contains about 100-200 milliliters of a suspension of these cells and is administered intravenously.
- And this is a one-time procedure?
-There are descriptions of repeated cell applications, but they are still quite limited.
— How do the chances of a successful treatment result increase with this therapy, how does the survival rate of patients change?
— CAR-T therapy is used in situations wherewhen there is no alternative. That is, for situations of relapse and refractory diseases. When there is no other way to get the effect. Therefore, from the point of view of achieving a reduction in the tumor mass, this is practically a life-saving method for some patients who have these forms of malignant tumors. On the other hand, it is now known that at least the second generation of CAR-T cells requires further consolidation of the effect with bone marrow transplantation.
Refractory form of the disease- a form of the disease that cannot be treated (in oncology and hematology, this most often means insensitivity to chemotherapy).
— That is, for patients who will be prescribed this method in the near future, is this the last hope?
— Yes, in fact it is. But it cannot be said that this is a completely safe method. Therefore, it is used only in situations where there are no other safer treatment alternatives.
- You have already mentioned complications: how will they be dealt with and is there already an appropriate therapy?
— Neurotoxicity is not the only complicationtherapy with genetically modified cells. There is also cytokine release syndrome - now with the advent of COVID-19, almost everyone knows about this syndrome. But in general, the term itself appeared in the context of clinical studies of CAR-T cells. Before this, it was thought that it was just a fever, a combination of toxicity. It was identified as a separate syndrome after CAR-T cell research began. A clear connection with the introduction of cells was identified, the timing of the onset of these symptoms was always the same, and the symptoms had a certain spectrum.
Cytokine release syndrome (CRS)is a set of symptoms that candevelop as a side effect of certain types of immunotherapy, especially those involving T lymphocytes. The syndrome occurs when immune cells become activated and release significant amounts of cytokines into the body.
Cytokinesare small proteins that work ascellular messengers and directing the body's immune response. However, high levels of cytokines can trigger an increased inflammatory response in the body. It can cause harm and disrupt a number of body functions. In severe cases, CRS can lead to multiple organ failure and even death.
Neurotoxicity is a particular variant of the syndromethe release of cytokines, in which the basis of all life-threatening problems is an increase in vascular permeability due to the excessive production of various proteins (causing an increased inflammatory response in the body) by these genetically modified cells. The end result is that vascular permeability increases and fluid from the blood vessels passes into the organs, edema occurs, in particular swelling of the brain. These problems are present in 50–80% of patients, depending on which variant of the CAR-T cell construct is used in therapy. There are already international recommendations for the treatment of this syndrome, and the sequence of actions for this complication has been determined. In principle, this situation is worked out quite well.
“Treating thousands of patients a year—a quarter of St. Petersburg's budgetfor healthcare"
— How much does this procedure cost for a patient and who finances it now?
— Today in Russia there is noNo CAR-T cell therapy products have been registered. A preliminary estimate of the cost of the first product, which a foreign manufacturer is currently preparing for registration in Russia, is 21 million rubles. Naturally, no financial instruments exist yet to provide such expensive treatment. The program that we are planning is a stage of academic research, it is not a commercial product.
Alternative to factory production -production of CAR-T in specialized laboratories. This path, for example, has been taken by some European countries that do not have the means to pay for factory production. Cells created as part of such projects cost about 10 times less than factory ones.
I doubt that we will get a budget comparable tothe same as what is spent on factory CAR-Ts in the US and some European countries. Most likely, it is the option of producing cells in specially certified laboratories that is more suitable for us - for example, as in Spain, where a non-commercial and locally produced version of this therapy has been developed and used.
Therefore, we very much look forward tothe support of philanthropists in order to support this research and provide supplies. In the case of our project, the patient will not pay, but, on the other hand, it is impossible to attract state sources of funding because these are unregistered technologies, and many consumables for production do not have state registration for medical use.
- And if we talk about a hypothetical future: is there a chance that the state will somehow subsidize this type of therapy for patients?
- Apparently, over time there will be a limitednumber of quotas. But it is impossible to cover the need for all patients at the expense of the existing health budget. For one of the meetings, I calculated how much volume would be required at current prices. If you buy at the prices of factory producers, this is a quarter of the annual budget of St. Petersburg for health care. If a decision is made on local production in special laboratories, then yes, this therapy will be available to all those who need it: about a thousand patients a year require treatment.
- You said: "a thousand patients a year." Is it both adults and children?
- Yes, children and adults, but more stilladult patients. Because the treatment of these groups of diseases in children is more effective than in adults. With standard treatment, they are more likely to be completely cured, and in adults, due to the different biology of the tumor, the probability of a complete cure from the initial types of therapy is much less.
"Targeted therapy may be less effective than conventional chemotherapy"
- If we talk in general about the types of therapy against oncological diseases. Is medicine now moving away from chemotherapy towards targeted methods?
- In fact, this is a continuous process -the transition to targeted techniques, which actively began about 10 years ago, when new drugs began to appear. In some situations, targeted therapy is not as effective as classic chemotherapy. And it cannot be said that it is always less toxic; it has a known profile of complications, which is clear how to deal with.
Another thing is that there really are nosologies,where the successes are very large and where it is possible to completely, for example, move away from toxic treatment methods and conduct outpatient therapy. Such a breakthrough five years ago was the emergence of non-toxic therapy for lymphomas. Checkpoint inhibitors have emerged, for which James Allison and Tasuko Honjo were awarded the Nobel Prize in Medicine in 2018.
Checkpoint inhibitors are used inanti-cancer therapy. Tumors use special molecules—called immune response checkpoints—to protect themselves from the body's immune system. With the help of inhibitors, doctors activate the immune system, directing its cells to fight tumors.
Today there is a wide range of nosologiesor genetic variants of nosologies that allow this type of treatment to be used with a cure of more than half of the patients, at least, or with the achievement of a deep response from the tumor. Yet checkpoint inhibitor therapy has very limited side effects, meaning it is an outpatient treatment given once a month or every other week depending on the option.
— Can patients receive targeted therapy for free in Russia today?
- Yes, it, like diagnostics, is included in the programcompulsory health insurance. But, of course, one must understand that no healthcare system in the world can afford to provide everyone with all treatment options. We have to differentiate: somewhere stochastically, that is, randomly, somewhere the health benefits are taken into account, choosing the most adequate cost / effect ratio. That is, for example, when the same checkpoint inhibitors appeared, in some European countries they did not pass the qualification for the ratio of benefits and economic costs.
- And, it turns out, they do not use these drugs?
— Within the framework of state programshealthcare in some countries is not. There are very few states where all therapy options are supported in general. The main problem is this: now it is important for the manufacturer of the drug to prove that the drug works in principle. But in reality, this means that the lifespan can be extended by only a few months - and this is still considered the success of clinical studies, while curing the patient will not work. But it cannot be said that it is beneficial for the healthcare system to pay 5 or 10 million rubles for a person to live a few weeks longer. This ethical issue exists for all healthcare systems in the world, even the wealthiest.
Drug manufacturers have enoughshow this difference between a placebo and a drug in relation to some nosology in order to obtain marketing authorizations and start selling the drug. The academic community, for its part, is trying to cure the patient. And in order to do this, a whole range of measures is needed.
In the last lecture that I prepared, wecalled the "patient trajectory" of existing treatments. It is necessary in order to determine the biological properties of his tumor, to which potential drugs it may be sensitive, which combinations and which consecutive treatment methods to apply. That's all the drug companies don't do today.
— Are such studies carried out in Russia?
— Yes, of course, including the Research Institute. Gorbacheva conducts a fairly large number of such studies: both separately with us and in cooperation with other oncological centers.
“This is a utopia - a story that we can provide for ourselves with everything”
— And where, if we talk about geography, are drugs for targeted therapy produced? Is pharma doing this in Russia?
—In general, a law was passed stating that all foreigndrugs must be packaged in the Russian Federation. Therefore, formally, we produce everything quite well ourselves. Another thing is that the substance itself is produced outside of Russia. And we must understand that in general, not a single country in the world fully provides itself with medicines produced within the state, therefore this is a utopia - a story that we can provide for ourselves with everything. In any case, this is a competitive environment, and some drugs are developed and produced in one country, some in another. And it is very important that there is free access to all methods of treatment. The problem of restrictive measures translates into the fact that medical tourism to Turkey is 30% cheaper than to Russia. Simply because all drugs imported into our country go through the stage of customs duties, and there is no such thing in Turkey.
- And if it’s about production: are we able to produce such drugs? Is it possible that some clinic in the US will use our targeted drug?
“Well, that hasn’t happened yet. But now there are several good examples at the stage of clinical trials, I can say that there are up to 10 such examples in Russia.
But it's better than zero.And if we return to protective measures: how do you feel about the “second extra” rule? How can it affect, first of all, patients and the level of trust in our medicine?
- I can say that the level of trust is stillis growing, including from the side of medical tourism, for example, last year we had a patient from China. But I am not opposed to generics or biosimilars, especially if they are well made. We have been working with generics for many years and have not seen anything bad in terms of side effects from most drugs. Another thing is that the efficiency is often significantly less, but it is impossible to prove this. Therefore, including our clinic, we actively participate in programs when we are trying to draw the attention of the government to the problems of treating children, the use of generic drugs for children with cancer. Sometimes such substitutions are accompanied by some deterioration in treatment outcomes, but there are no mechanisms for withdrawing low-quality generics from the market.
- But as I understand it, with the “second extra” rule, both patients and the doctor simply have no choice ...
- Rather, there should be a decision on the statelevel on the need to create a strategic list of drugs, the quality of which should be controlled. Because it cannot be said that even before the patient had a choice: oncological care basically belongs to the category of state free medicine. A very small percentage of people can afford oncology care out of their own pocket today. Who can afford therapy for 21 million rubles, as in the case of CAR-T?
“It takes at least five years to introduce a new treatment method”
— How does charity help in research today?
- Funds about half of all researchin the field of cancer treatment. And there are several problems here. First, academic research involves several stages. Diagnosis requires methods and studies that do not yet have registration certificates. That is, we cannot spend on them the money that the state allocates. Since such methods appear very quickly - in 2-3 years, the approach to modern diagnostics of malignant tumors changes dramatically - the manufacturers of these reagents are not interested in registering their product, going through this long path that takes about a year or longer. Accordingly, the only option is charity.
Secondly, these are still drugs that canbe used outside the scope of registered indications, for new indications, or is it such a rare story that drug manufacturers simply do not register certain indications: it is not economically profitable for them. And in this case, we also cannot use public money.
REFERENCE
Charitable Foundation AdVitasince 2002, she has been helping adults and children who are being treated for cancer in St. Petersburg clinics and oncology departments of hospitals.
The task of the foundation is to make modern treatmentavailable to anyone regardless of age, income level, medical prognosis. We help at all stages: from diagnosis to completion of treatment. AdVita pays for diagnostics, medicines, search and activation of bone marrow donors, equipment, reagents and consumables for clinics, and supports scientific research.
You, too, can help Russian scientists develop new types of therapy and, as a result, save thousands of lives:
I WANT TO HELP
- How is the introduction of new methods, if we talk about therapies for oncological diseases: from the laboratory to the specific doctor who will apply the new method?
— There are two types of clinics — academic andmunicipal health care. The latter, according to current orders, cannot initiate any research themselves. Therefore, they work within existing treatment standards and clinical guidelines. Academic clinics, by which I mean scientific and educational institutions, can initiate research. And the results of their research can then form the basis of national recommendations, which we must update every two years. Already on the basis of these recommendations, municipal clinics apply a new method of treatment, which has shown great effectiveness. Since a small number of academic studies are being conducted in Russia, the results of American and European working groups are more often broadcast, which are also then included in clinical recommendations and treatment standards.
— How is communication between developers arranged?treatments and practitioners? Can a conditional doctor from Samara call St. Petersburg and ask: I am using your therapy, something is going wrong with me, what should I do?
- In general, we are trying to come to such an option andto create working groups regarding specific problems in the field of oncology and hematology, where communication would be open between all parties involved. Because it is a known fact for any field of human activity: the more communications, the better the result.
- And how long does it take for a full cycle from the beginning of the development of therapy to its implementation?
- At least - about five years, because now,of course, treatments are approved simply by response rates, but more often than not, the standard is to estimate the proportion of patients in whom the tumor does not progress after 2–5 years. Accordingly, you need to wait, observe the patients and determine how effective this or that method is.
— What areas of cancer treatment can be called the most promising?
- It is clear that new drugs will appear.The next generation of drugs will be based on the activation of the capabilities of a person's own immune system, and this is already happening. We literally every year have a new drug for some kind of disease that uses a mechanism that is based on helping immune cells cope with the disease. And, of course, genetic modification of various cells of the human body will be more actively used.
— What is the role of Russian science in these developments?
- The role of a very seriously catching up participant in the process.
What would you call your professional mission?
— When I went to college, I had oneof such fantastic ideas: to try to completely overcome cancer. And then, when I started working, I realized that this was a complete utopia. But in some areas it turns out to move this problem a little further. And, perhaps, it gives pleasure, but, of course, any person in any profession will tell you that 90-95% of life is routine work.
Read more
NASA invites you to see the photo that Hubble took on your birthday
The experts said that the sixth generation fighter hit the satellite images
See what the James Webb telescope looks like from Earth